Faster, stronger, higher
Can a 3-week outpatient programme in an 'enriched environment' work for those who have experienced brain injury. Billy Mann finds out
Who? People affected by brain injury who might benefit from some focused therapy.
What? A three-week intensive programme of physiotherapy and occupational therapy.
Where? National Hospital for Neurology and Neurosurgery, Queen Square, London.
When? January 2015.
Why? Therapy in an 'enriched environment' can lead to unexpected positive outcomes.
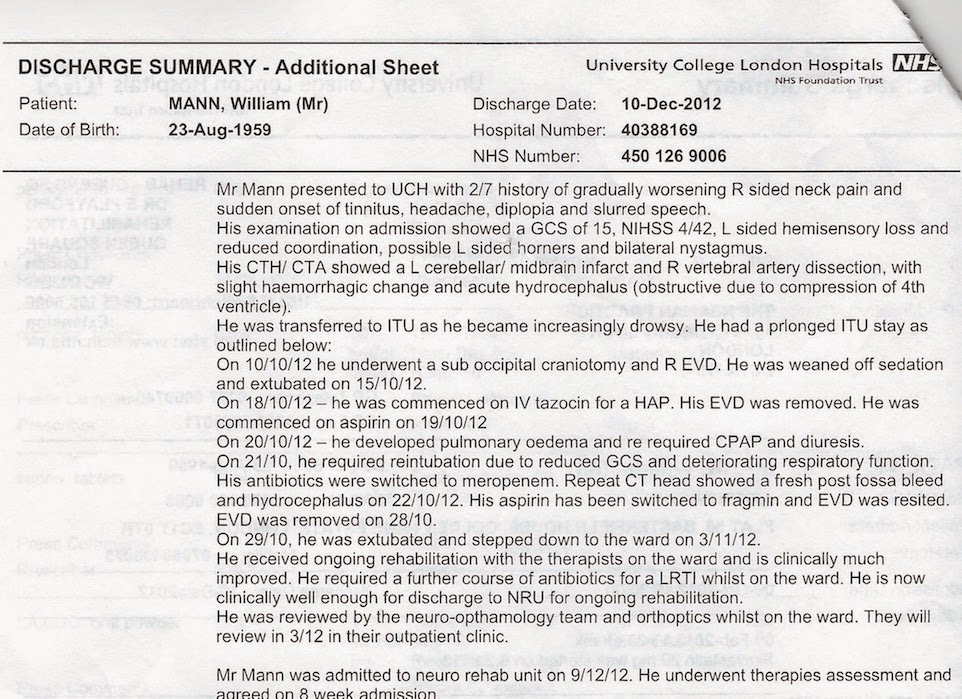
27.01.15 It is two years since I was discharged from the
National Hospital for Neurology and Neurosurgery in Queen Square, London, following a 'bleed' stroke. A lot has happened since, but right now the situation is this: I am doing a three-week intensive
Upper Limb Bootcamp of physio- and occupational therapy. After one day of assessments and form filling (yesterday), I am on a regime of doing stuff with my left hand only. The idea is that, slowly, the speed and dexterity in my left arm and hand will increase so that eventually that limb will become a more useful partner in the to-ing and fro-ing of everyday life.
 28.01.15
28.01.15 Left-hand typing when you are right-handed is a revelation on many levels. First and most obvious, it is about six trillion times slower. But during the painstaking process you have so much bloody time on your hand(s) that you are able to consider other, more nuanced factors that play role in what is seen as a routine task. Take, for example, that last sentence. In the time it took me to tap it out, I revised the choice of words and their final formation into a sentence about six times. Yes, and it is still rubbish. And then I noticed how often I miss out the letter ‘i’ from some of the words that are meant to contain it. Now corrected.
This might be considered a good thing. ‘The secret of style: knowing what you want to say, and knowing how to say it.’ That’s what
Somerset Maugham said/wrote, though I suspect he would never have put that comma before the word and. In other words, by slowing the process to snail-pace you have more time to consider properly what the hell it is you want to say. This must be what it is like to be
Stephen Hawking.
29.01.15 Day 4. One thought that has crossed my mind is that ever since I was discharged from NRU (Neuro Rehabilitation Unit) two years ago, I have driven the idea that bilateral is best. I have pursued and participated in activities that engage the use of both hands at the same time. Gardening is a good example. Potting, pruning, labelling plants, digging and cleaning: it’s all good, wholesome bilateral stuff with both upper limbs pulling their weight, even if the right does a bit more work than the left. But in forcing myself to do things left handed (I am naturally right handed and my right side is the stronger) I not only give my right side a holiday I am hopefully equipping my left side to do a bit better in the future.
So, in following this regime of torture (the urge to bring my right hand to the party is very strong), maybe I will become better at being bilateral. I sometimes close my eyes and give thanks that the stroke disabled my weaker left side rather than my stronger right side. I imagine that this is what it would be like had things happened the other way round.
Left-handed eating is a mixed blessing. The excruciatingly slow pace presumably makes for a slower, healthier digestion. Good thing, that. For me, spearing with a fork is slow but, with effort, successful. Scooping, however, is laced with danger and makes me nervous. Bad thing, that. In the ‘outside world’ I would be terrified of embarrassing myself and any of my dining companions by catapulting assorted meat and veg all over the place, but here in NRU that kind of thing is just a part of the everyday orgy of dysfunction.
02.02.15 The weekend went well and I managed to build some of the new processes into my routine. Typing and eating and drinking left handed continue to be laborious, but small improvements in performance are noticeable. Frustrating though it is, I can feel a change. I suspect that much of it is to do with confidence, and it is best seen when I allow my left and right hand to resume their natural partnership.
 03.02.15
03.02.15 Physio Jo says the shaking in my left hand might be reduced by strengthening my left shoulder. She says my left shoulder exhibits 'winging'. We tried a couple of exercises - the 'dart', in which I lie flat on my front and attempt to pinch my shoulder blades together in a sort of rotation, and a yoga pose called the 'cat', in which from a kneeling position you raise and arch, then collapse your back in the moggy style. I think I have got the hang of the 'dart', but 'cat' will take a little more work.
04.02.15 More effort trying to get me in touch with my shoulder blades. With time I am sure it will come. Given that, until two days ago, I was hardly aware of their function, this is progress. Also tried carrying a cup of coffee in my left hand, but given the mopping up I had to do afterwards, this needs more practice.
Look, I made a clay brain in arts and crafts. Ronnie [Sharon] did a flower arrangement
05.02.15 Just getting here on time today seems like a substantial achievement. A bus strike forced me to improvise an alternative route using those sardine bullet trains they call the London Underground. The final stage of my journey involved an out-of-action second lift at Russell Square's ultra-deep station. But arrive I did, and continued the struggle to disentangle some old hunching habits from my left shoulder blade. In a pathetic attempt to seize some momentary respite, I asked physio Jo what muscles we were working on. The only word I can remember is 'subscapular', which I am sure means something to someone other than me. Then it was a quick pre-lunch bit of OT circuit training with Caroline - emptying the dishwasher and storing items in the cupboard, walking up and down stairs, and my GREAT FAILING of carrying a cup half filled with liquid in my left hand from A to B and back again ad nauseum, till the end of bloody time, etc.
At lunch, my bootcamp co-conspirator Steve attempted to impress nursing assistant Emma by warning her that the only reason I am in the gym so often is that I need to practise shinning up drainpipes and climbing through windows. Emma (from Birkenhead) told Londoner Steve that he ought to be ashamed of himself stereotyping Liverpudlians in such a negative way. Or words to that effect. I left them to it and returned to the gym, where physio Jo put me through a series of exercises (two variations or derivatives of the 'dart', something with a glorified elastic band tied to a rail, and kicking a very large plastic ball against a wall using both left and right feet) which I am optimistic of taking with me into the outside world.
06.02.15 Continuing the new exercises in an attempt to find a way of building them into my daily routine. Most of them - rubber band work, ball work - will be easily embedded into my current gym programme. But improvements in the flexibility and strength of my shoulder blades can only really be seen by a physio, even though I believe I can already feel the benefits. This means that the race is on to find a do-able routine for me. I am confident that physio Jo will pull a rabbit out of the hat, but right now I seem to be failing a lot of tried and tested ideas. The out-order lift provided the golden opportunity to practise my stair walking, and three times round Queen Square Gardens swinging my arms while attempting to walk like John Travolta.
08.01.15 Just been for a swim (six lengths, plus stretches) and afterwards reflected on why I so seldom do it when it is so easy and close by. I have been using the excuse that is a) a lot of faff, with lockers and getting changed, etc, and b) potentially dangerous, or at least precarious, poolside, what with the wet surfaces and my poor eyesight, etc. This is all classic avoidance bollocks. Going for a swim is actually a very good combination of physio and OT. So long as I can recast the so-called 'faffing' as OT, all I need to do is set aside an hour in which that is WHAT I WILL DO NOW, in much the same way I set a time each day to complete the GRASP exercise routine.
09.02.15 Shirt buttons are still a bit of a pig for me, especially doing up the right cuff with the left hand. Inevitably, a lot of shaking kicks in. Then I try to concentrate on stopping the shakes but end up overthinking it and thus shaking even more. Caroline has told me to stop when that happens and to gently shake my left arm and wrist. But overthinking is one of my big weaknesses, especially when it comes to OT and physio. Until I learn to properly let go and chill, plasticity will be inhibited. A good example came in the physio session that followed. Getting my arms to swing in coordination with my legs while walking is clunky and difficult. Physio Jo watched me in action and said I should try to sync left arm with right leg and vice-versa. Physio Anna was watching and started to walk alongside me. As soon as I got the correct rhythm going, she started to ask me questions about my weekend. This distracted my attention and I stopped thinking AND JUST DID IT. Now all I need is some way to fly solo using the same technique. Maybe I should revisit some of my favourite poems. So ...
What passing-bells for these who die as cattle?
Only the monstrous anger of the guns.
Only the stuttering rifles' rapid rattle
Can patter out their hasty orisons
Not showing off, or anything, but in a 3-way Wii bowling competition (Me, Theresa and Steve), I won, though to be fair Theresa scored most strikes.
10.02.15 Struggling to button my shirt this morning I began to wonder whether I had subconsciously acquired an avoidance of shirts with buttons because of my left-limb difficulties. This is possible, even though I think I have always favoured pullover style top clothes (T-shirts, sweatshirts, jumpers). In fact, I wear buttoned shirts (often with tie) more often now than I have ever done in my adult life. But I definitely need to practise the buttoning thing more often. In repeatedly buttoning and unbuttoning my shirt in 20-minute relays with exercises in carrying beakers half filled with water, I wondered whether the theory expounded in Malcolm Gladwell's book Outliers, in which 'success' can be had for the small sum of 10,000 hours of repetition, has any application to the treatment of brain injury. At my daily circuit doing the John Travolta arm-swinging walk around Queen Square Gardens I repeatedly recited Edward Lear's The Owl and the Pussycat to embrace Anna's 'cognitive distraction' method of everyday physiotherapy.
 Look, I painted my clay brain. Badly
Look, I painted my clay brain. Badly
11.02.15 More buttoning today. Must wear proper shirts more often, then I would be able to do this exercise while watching Midsomer Murders and counting the bodies. I have started to make a list of the routines I have followed while here so that I can hopefully devise an actionable afterplan. At the moment it includes three physio elements, three OT and three that are cross-discipline, so to speak. The OT areas are: Shirt buttoning left handed, carrying a cup half filled with water left-handed. Plus drinking left-handed. And last, emptying the plastic dishwasher cutlery unit left handed and storing the contents in the correct kitchen drawer slots. On the physio to-do list are: walking with no stick, arms swinging - faster, faster, faster; ball bouncing and kicking; building shoulder strength with the glorified rubber band, and attending yoga or pilates classes to master the 'Cat' and 'Dart' poses for my shoulder blades. Plus prod the door with shoulder blades to strengthen. The dual physio/OT items on the list are: swimming, GRASP exercises and walking up and down stairs or steps without using the rails. Jo and Caroline will feed back to me on those and we will devise a plan at the end of this week.
12.02.15 To Tutti's in Lambs Conduit street at 9am for a meet with physio Katie Campion and Lu from Bridges to discuss a 15-minute slot at a goal-setting conference here at the National in April. Then back to NRU for a quick gym circuit and a group GRASP session with Steve and Nicola. After lunch it was Wii table tennis with Paul and Steve, supervised by Mavis, who showed great patience and fortitude in the face of Steve's raunchy banter. Oh, did I mention that I won? Cleaned up, in fact. Happy days. I am beginning to detect what my week links will be after this week. Number 1 is cup carrying left handed.
13.02.15 The last day and it is not just time to revisit tests, goals and outcome measures, etc, but to reflect on the past three weeks. From a health point of view, I have been treated to a remarkable reawakening of the physio and occupational therapies that have and will continue to be part of my everyday life. Many of these have already been mentioned in this blog, but what I do with them from here on is a state-of-mind issue. I can't say I will miss the restriction/constriction of my right hand that required me to type only with my left hand. I will miss the pause for thought that restriction/constriction placed on me that resulted in a better choice of words and sentence construction. But, to be frank, typing on a phone touchscreen with your left hand only is rubbish. I breezily stated during one conversation somewhere along the line that "Bilateral is best. We have two arms, hands, ears, legs and feet for a reason." And yes, I think that is true. So, one of the biggest challenges I face now is not physical but psychological. Among the words most often used by my therapists over the past three weeks are, "Billy, you are overthinking this. Stop analysing." This is easier said than done, especially in my case. But I would say that, wouldn't I? Yet in those rare moments when I stop doing what I call "a Woody Allen" (overthinking), I sort of glimpse a different self, and one I think I like a bit more than the one I am now. So there is even a bit of self-love to be unearthed if I can stop being so annoyingly pensive.
At this point I am reminded of the last time I was here at NRU, 2 years ago. There was one day, after weeks of successful evasion on my part, that I was boxed into a corner by the hospital chaplain. "Bugger," I thought. "I've been dogcollared." And that word, "Dogcollared", became the title of a short 10-minute play/sketch I then began to write about a neuro patient who is cornered by the hospital chaplain and proceeds to interrogate and bait him on the existence of God so intensely that the poor chaplain (who the patient stupidly keeps referring to as Charlie) has a stroke. But at least he was in the right place, etc, yadda yadda. And this latest visit has had similar effect. In this story a gang of neuro therapists, led by a speech-and-language clever clogs, set out on a quest to find out what Stephen Hawking's real voice sounded like. Obvs, when I say real I mean pre-machine. On the way, two of them fall in love listening to early cassette tapes of Hawking muttering to himself about dark matter, or something. A winner, huh? See you at the Oscars. Remember where you heard it first.

{kind=link}